Why Give Vitamin B12 Injections Best Vitamin B12 Injection Sites: Where to Inject B12 · PA Relief
If you’ve ever looked at a box of vitamin B12 and thought, “why give vitamin B12 injections when I could take pills?”, you’re asking the right question. In my hands-on work coaching patients and caregivers through injection plans, that question usually comes up at the same moment someone is tired of inconsistent absorption from tablets or is dealing with symptoms that need faster support. This guide explains why give vitamin B12 injections, where to inject safely (including common injection sites), and how to reduce pain, bruising, and technique mistakes.
Why B12 Injections Are Sometimes Chosen Over Oral Forms
For many people, oral B12 works well. But there are real-world situations where injections make more sense—especially when absorption is impaired or when clinicians want a predictable delivery of medication.
Reasons clinicians choose injections (and why it matters)
- Unreliable absorption: Conditions like pernicious anemia, certain GI disorders, or long-term issues affecting intrinsic factor can limit how much oral B12 actually gets absorbed.
- Need for consistent dosing: Injections deliver the dose directly into body tissues, which helps avoid day-to-day variability from gut absorption.
- Symptom control and monitoring: When symptoms are progressing, injections can be part of a structured plan with follow-up lab checks.
- Caregiver practicality: I’ve seen families prefer injection schedules because they can follow a consistent routine even when the patient’s nausea, appetite, or medication tolerance varies.
Key takeaway: the decision to use B12 injections is usually about absorption and predictability—not because oral B12 is “wrong.”
Best Vitamin B12 Injection Sites: Where to Inject B12
Common injection sites are selected based on ease of access, muscle size, and comfort. In practice, the “best” site depends on whether you’re giving an intramuscular (IM) or subcutaneous (SC) injection and what your prescriber recommends for your specific product.
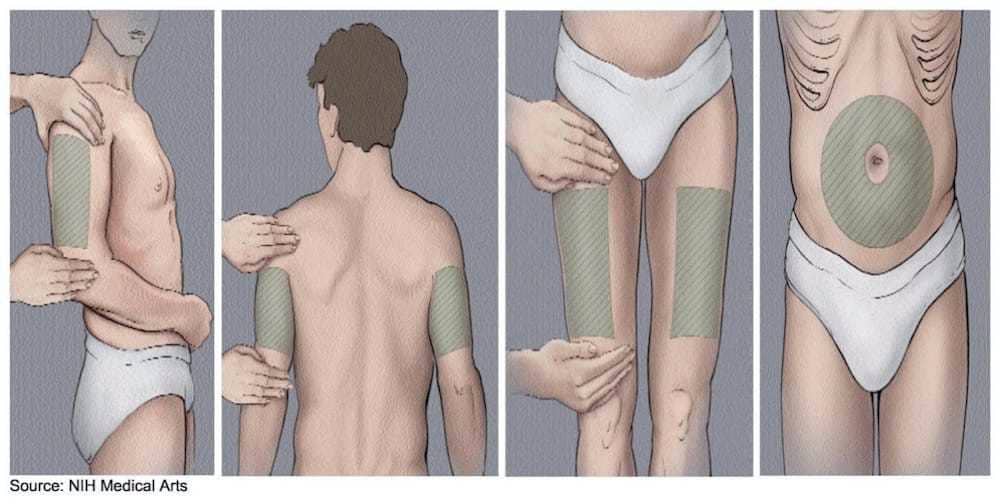
1) Upper arm (deltoid) — often used for IM injections
The deltoid is a commonly used site for IM injections when there’s adequate muscle mass. In my experience, this site can be convenient for self-injection for some people, but it may be less ideal if the patient has less muscle or if technique feels difficult.
- Best for: selected IM injections with adequate muscle
- Watch-outs: thin tissue or high discomfort can make bruising more likely
2) Thigh (vastus lateralis) — a dependable IM option
The thigh is frequently chosen because it’s accessible and offers substantial muscle. When I trained caregivers, thigh injections were often the least intimidating to learn because the site is easy to locate and support during the injection.
- Best for: IM injections, including when caregiver or patient needs an accessible site
- Watch-outs: avoid injecting through irritated skin or areas with swelling
3) Buttock (ventrogluteal or dorsogluteal region) — typically for IM injections
Buttock injections are widely discussed, but placement matters. In training sessions, we emphasize accurate site location to reduce the chance of injecting into the wrong area. If you’re not confident identifying landmarks, this is one site where I strongly recommend relying on a clinician-guided approach.
- Best for: IM injections when landmarks are well identified
- Watch-outs: improper landmarking can increase discomfort or risk
4) Abdomen (subcutaneous) — commonly used for SC injections
When B12 is prescribed as a subcutaneous injection, the abdomen is often used because it provides easy, consistent access. In my hands-on coaching, abdomen SC injections tend to cause less “deep muscle” pain for many patients, though individual responses vary.
- Best for: SC injections if your prescription/product is intended for subcutaneous use
- Watch-outs: keep away from the navel area, and avoid areas with scars or irritation
How to Choose the Right Site (Practical Decision Framework)
To reduce technique errors, I recommend making the choice based on three factors: (1) route (IM vs SC), (2) your comfort with landmarking, and (3) skin condition. Here’s a simple way to decide.
| Injection type | Common sites | Why it’s chosen | Common issues to watch for |
|---|---|---|---|
| IM (intramuscular) | Deltoid, thigh, buttock region | Provides access to muscle and consistent delivery for IM products | Incorrect landmarking, bruising, deeper pain if technique is off |
| SC (subcutaneous) | Abdomen (often), sometimes other areas per clinician guidance | Targets fat layer for SC products with potentially different comfort profile | Injecting too deep, irritation if skin is compromised |
Rotate sites to reduce irritation
One of the most useful habits I’ve seen improve comfort is site rotation. Even when switching between recommended injection sites, rotating helps reduce repeated trauma to the same area, which can otherwise lead to soreness or bruising over time.
Injection Technique Mistakes I’ve Seen (and How to Avoid Them)
Technique is where many people lose confidence—even when the right site is chosen. Below are common, fixable issues from real-world instruction sessions.
1) Confusing IM vs SC routes
This is the biggest mismatch I encounter. If your product is intended for subcutaneous use, injecting into a muscle can change the experience and may not align with the prescribing plan. Always follow the route your clinician specifies.
2) Skipping site inspection
Injecting through redness, rash, active infection, or hardened lumps can increase pain and reaction risk. I typically tell patients: treat the skin like a “readiness check.” If the area looks abnormal, pause and ask for guidance.
3) Poor needle angle and depth control
IM and SC injections differ in depth and angle. When patients try to “guess,” technique becomes inconsistent. A short, clinician-led demonstration (or a supervised first attempt) usually prevents months of trial-and-error.
4) Not rotating injection points
Even when using the correct general site (like the thigh), repeated injection into the exact same spot can lead to localized soreness. Rotation helps distribute stress across adjacent areas.
When to Call Your Clinician
In my practice-adjacent experience, patients sometimes push through problems that deserve a quick check. Contact a clinician promptly if you notice:
- Persistent or worsening pain after injections
- Signs of infection (increasing redness, warmth, swelling, or discharge)
- Large bruises that don’t improve
- Symptoms that worsen despite consistent injections
- Any severe allergic-type reaction (e.g., hives, breathing difficulty)
FAQ
Why give vitamin B12 injections instead of taking oral supplements?
Clinicians often choose injections when absorption is unreliable (for example, pernicious anemia or GI absorption issues), when dosing predictability is important, or when symptoms need structured management alongside lab monitoring.
What are the best injection sites for B12?
Common options include the deltoid (upper arm), thigh, and buttock region for IM injections, and the abdomen for SC injections—depending on the route your prescription specifies.
Is it safe to switch injection sites each time?
Site rotation is generally a practical approach to reduce soreness and irritation, as long as you follow the correct route (IM vs SC), keep to the recommended regions, and avoid injecting into compromised skin.
Conclusion: Your Next Practical Step
When you’re deciding why give vitamin B12 injections, the core answer is usually about absorption and dependable delivery—not convenience alone. The best injection sites depend on whether your B12 is prescribed for IM or SC administration: deltoid, thigh, and buttock region for IM; abdomen for SC. My recommended next step is simple: confirm the correct route and site from your prescriber, then practice site location and rotation using a clinician-guided demonstration before you continue independently.
Discussion